
Content verified by

Some children live with conditions that affect their bladder capacity and pressure, leading to discomfort, infection, urine leakage, and risk to kidney. To help these children live a normal life free from the worries of urine leaking or kidney and bladder infections developing, our specialist urology department at Evelina London Children’s Hospital offers life-changing treatment; bladder augmentation and the Mitrofanoff procedure.
Symptoms and causes
What conditions can affect a child’s bladder function?
A child’s bladder function can be affected by several different conditions. Often, these conditions are picked up before birth during a pregnancy scan but, in other cases, they may be detected in young babies who present with regular urine or kidney infections. Common conditions which can cause bladder problems in children are:
- blockages in the urethra (the passage through which urine passes to leave the body)
- spina bifida (and other spinal conditions or injuries)
- anomalies affecting the anus and rectum
- functional bladder problems.
What are the symptoms of bladder problems?
Some of these conditions may lead to a child having a very small bladder which is unable to hold normal amounts of urine. A smaller bladder also typically means that urine might be held at a very high pressure which is known to trigger infection, leakage or kidney damage.
In children with spinal conditions like spina bifida, the nerves in their spinal cords that are responsible for controlling the bladder are affected. This can lead to these children struggling to store urine in their bladders or to empty their bladders completely. Some children are even affected by both of these issues at the same time.
Children with anomalies affecting their anus and/or rectum often have an effect on their bladder activity. This severely impacts their quality of life and the condition may require surgical treatment.
Some bladder anomalies in children can often be detected prenatally at a routine pregnancy scan. If this is the case, you will be connected with a team of specialists to help you prepare for what to expect once your baby is born, and to discuss potential treatment options for them.
If a bladder anomaly is not picked up before birth, it can be detected due to bladder infections, kidney enlargement and regular urine leakage.
What happens in the Mitrofanoff procedure?
The Mitrofanoff procedure was described in 1976 by Professor Paul Mitrofanoff as a way to essentially reroute urine through a new channel (called a Mitrofanoff) from the bladder directly to the abdomen wall. The Mitrofanoff is created from the child’s appendix or, if they have no appendix, a little piece of their small intestine.
Your child will need to be under general anaesthetic for the duration of the Mitrofanoff procedure. The surgeon disconnects the appendix from the large intestine and uses this as a tube to connect the bladder to the abdominal wall. If the child has no appendix, at this stage the surgeon will instead take a piece of the small intestine to convert into a tube and connect this in the same way as the appendix is used.
The Mitrofanoff channel creates a valve which prevents urine from leaking out of the bladder. Instead, your child will need to use a catheter (a narrow tube) to drain the urine from their bladder by inserting the catheter into the Mitrofanoff opening.
Catheterisation is a quick process and our team of paediatric nurse specialists teach children and family members to do this. Most of our young patients adapt well to life with a catheter and are able to perform the process independently.
Although in most cases the Mitrofanoff procedure is performed in the same operation as a bladder augmentation, in a selected group of children, bladder augmentation is not required and the Mitrofanoff procedure can be performed without it. If a bladder augmentation is not needed, the Mitrofanoff procedure can even be performed as keyhole (laparoscopic) surgery.
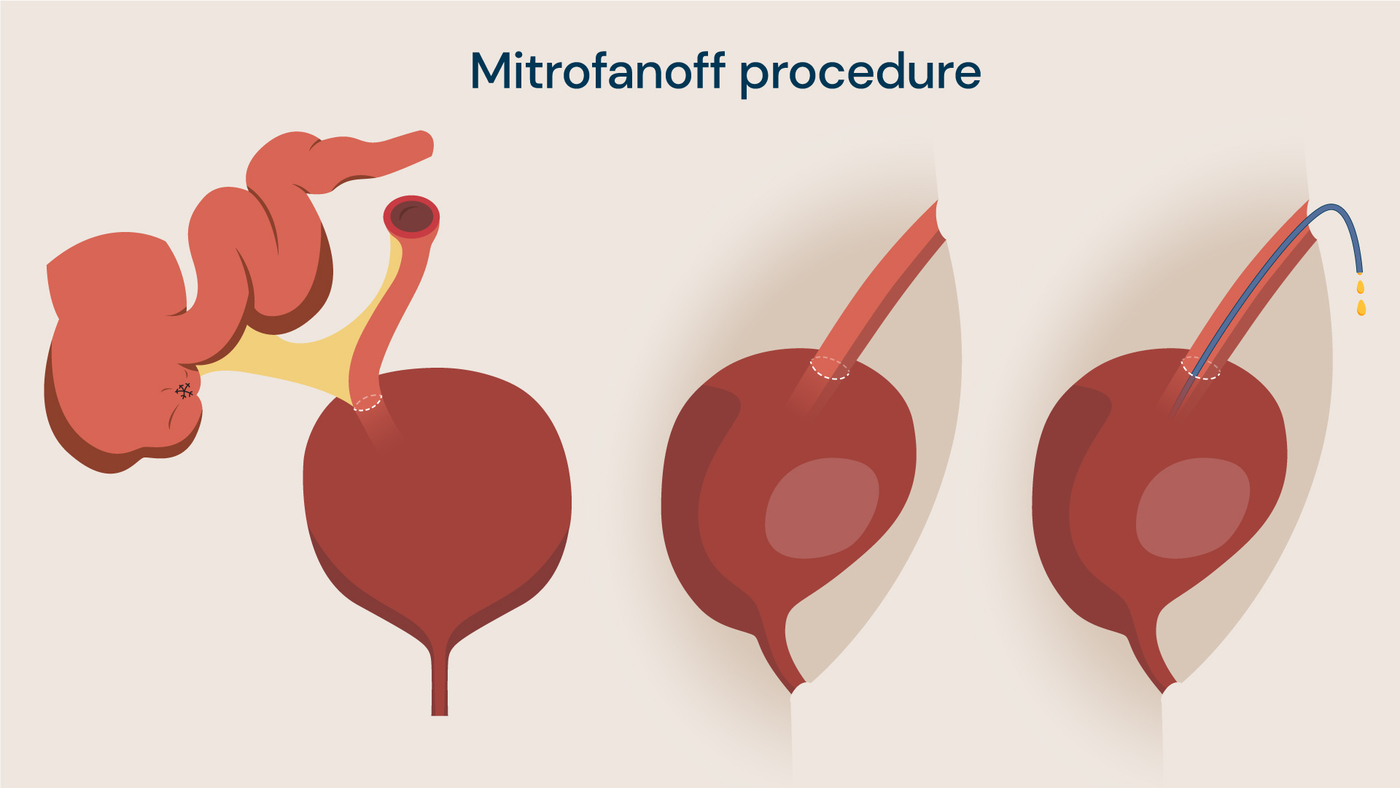
A tube is created from the appendix or small intestine (left) which connects the bladder to the outer abdominal wall (middle), allowing urine to be drained through a catheter (right).
What happens in the bladder augmentation procedure?
Some children may also require another procedure at the same time, called a bladder augmentation, to enlarge the bladder and increase its capacity. This also helps to reduce the pressure at which urine is held in the bladder, minimising discomfort, the risk of infection, and damage to kidneys.
To carry out the bladder augmentation part of the surgery, the surgeon opens up the bladder and forms it into a shape a bit like a cup. Then, they use tissue from the bowel to create a lid-like structure to cover the top of the bladder and join the two together, forming a bladder with increased capacity.
As with treatment for any condition, surgery is the last resort after medical management has failed. Before having bladder augmentation surgery or the Mitrofanoff procedure, alternative treatments should have been explored. These include bladder relaxing medications or Botox injections to help the bladder empty fully.
If the bladder does not respond to these medications and cannot be drained by self-catheterising through the normal channel, then surgical interventions such as bladder augmentation and the Mitrofanoff procedure can be considered.
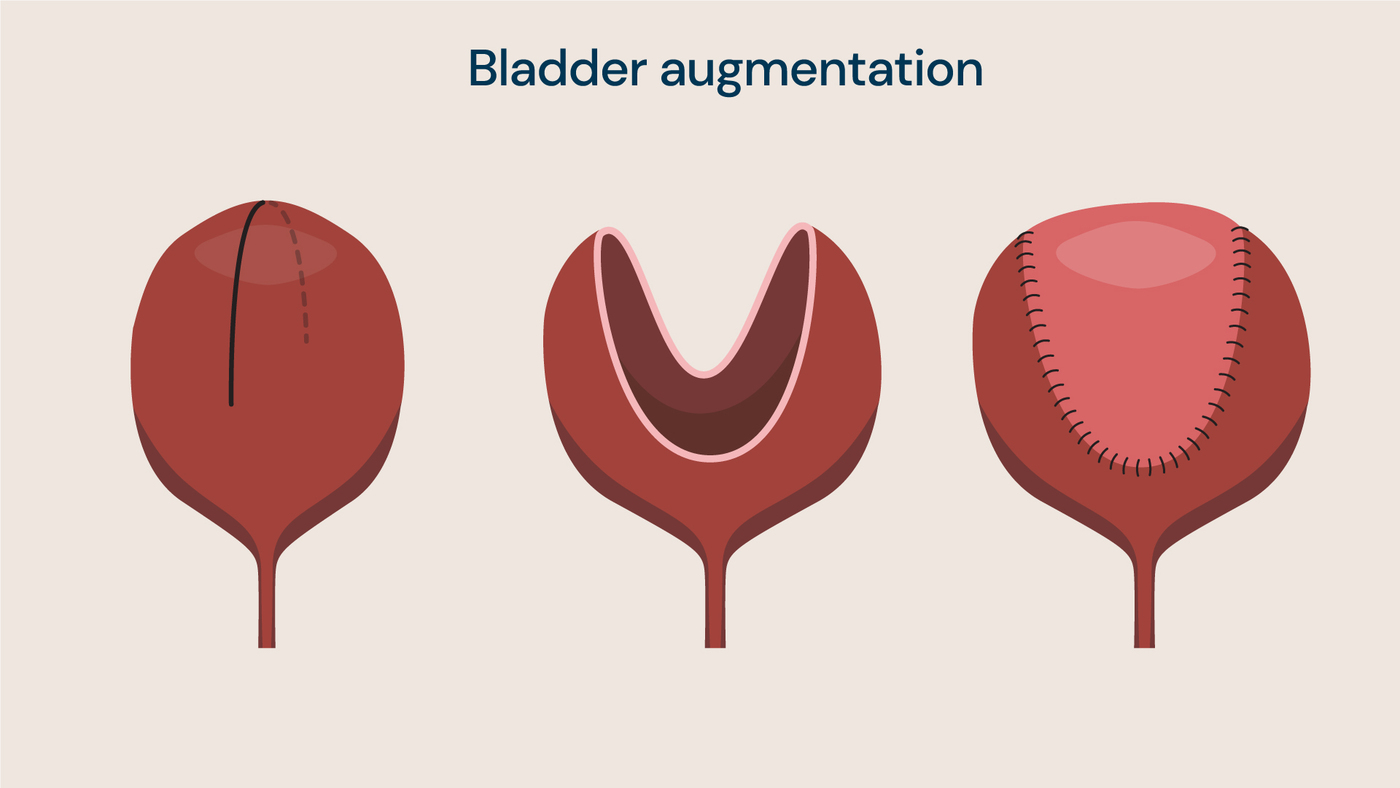
The bladder (left) is opened up during the procedure (middle) and a piece of bowel tissue is stitched onto the bladder to increase its size and capacity (right).
Preparing for surgery
As with any surgery, preparing for the Mitrofanoff procedure and bladder augmentation must be done carefully with expert guidance from our team of specialists at Evelina London. Prior to surgery, you and your child will meet with the surgeon and clinical nurse specialist and play therapists to discuss the surgery and understand what to expect on the day.
The surgeon may give your child a bowel preparation diet to follow, although this will vary from patient to patient. It is important that you follow any instructions given and understand what the operation and postoperative care involves before going ahead with surgery.
After surgery recovery
After the surgery, your child is likely to stay in hospital for from 2 to 7 days, depending on the type of operation, so that our urology team can monitor their recovery and ensure they are healing well before they return home. During this recovery period, and for up to a month after the surgery, your child’s Mitrofanoff will have a catheter left in it to allow the tube to stay open. Leaving the catheter in means that the Mitrofanoff can heal in a way that ensures your child, later in their recovery process, can insert a catheter easily to drain their own urine. In addition, there may be an extra tube in the bladder and urethra if an augmentation surgery has also been carried out.
When the surgery wound has healed well, you and your child will attend another appointment with our urology specialist nurses and be taught how to catheterise using the Mitrofanoff. In the initial period, you will also be taught how to cycle your child’s bladder by clamping and releasing the catheters. You and your child will also have a follow up appointment with the surgeon around three months after the operation, followed by annual check-ups thereafter to provide regular monitoring and care.
Your child will be assessed with kidney function tests, kidney ultrasounds, urodynamic studies and blood tests to check that everything is working well and that their bladder and Mitrofanoff channel are healthy.
How to use a catheter
Using a catheter is straightforward and most children adapt well to life with a Mitrofanoff, especially when taught catheterisation techniques by our urology specialist nurses and play therapists.
Before beginning catheterisation, you and your child must wash your hands thoroughly. The end of the catheter which is entering the Mitrofanoff must be lubricated (if the catheter is not pre-lubricated). Then, you or your child can gently insert the end of the catheter into the Mitrofanoff opening and carefully guide it into the bladder. You shouldn’t need to apply too much pressure.
Allow the urine to drain from the tube into the toilet, and slightly move the catheter in the bladder to ensure that all urine has been drained. When you are sure that the bladder is empty, you can remove the catheter, before disposing of it or washing it ready for the next use (if it is a multi-use catheter). This must be completed approximately every three hours to keep the bladder empty and reduce risk of infection.
Benefits of bladder augmentation and the Mitrofanoff procedure
The Mitrofanoff procedure has numerous benefits for children who have the surgery and can be life-changing for several reasons including:
- minimised risk of infections
- reduced discomfort
- ability to be socially dry
- ability to independent empty the bladder
- safety of kidneys.
For children who have previously dealt with constantly leaking bladders, the bladder augmentation and Mitrofanoff procedure allows them to live life normally without the worry and discomfort caused by regular leaking and infections.
Further to this, the opening made on the abdomen through which the catheter is inserted is very small and can even be hidden in the bellybutton. It is mostly unnoticeable to others, so children with a Mitrofanoff have minimal outward physical difference from children with fully functioning bladders.
Risks of the Mitrofanoff procedure and bladder augmentation
The Mitrofanoff procedure and bladder augmentation are very safe surgeries but, as with any surgery, there are some risks. Most of these risks will apply to any surgery and include:
- infection
- internal bleeding
- urine leak
- narrowing of the Mitrofanoff channel
- allergic reaction to anaesthetic.
During the surgery, urine can also leak internally into other areas of the body and lead to irritation. The is also a small risk of internal bleeding when the appendix is disconnected from the intestine, before it is reattached to connect the bladder and abdominal wall.
The other risks associated with the Mitrofanoff procedure come after the operation and relate to catheterisation. There can be problems with catheterisation including infections, but difficulties using a catheter can usually be resolved by opting for a smaller catheter or more lubricant. Your child will also receive antibiotics while they recover to minimise the chance of infection.
Additionally, in cases where part of the small intestine is used, your child may experience excess mucus in their urine. This will require regular bladder washouts to prevent the formation of bladder stones. If this bladder cycling and drainage is not carried out appropriately, it may lead to contraction and failure of the bladder augmentation.
Most children will require an additional procedure later in life to adjust the new tube created from the appendix, or to remove growing scar tissue which can block the Mitrofanoff channel. Having regular check-up appointments over the years after the initial surgery will highlight these issues and ensure that your child receives further treatment when they need it.
As with any abdominal surgery, there is a risk of sticky bowel and bowel obstruction, especially after such a major operation. Your consultant can tell you more about what to do, should this occur, and provide following up care if required.
Locations
Our expert children's urology team see patients at the following locations:
Our children's urology experts
If your child has problems with their bladder function, has high bladder pressure, or regularly experiences urine and kidney infections, you can contact our expert urology team for an appointment.